


Values & Policy Initiative
This article is part of our Values & Policy Initiative, a six-month long process for the community to come together to learn and discuss our core values, tactics and positions so that we are more unified in our work as a large, diverse community. This process will culminate in a statement of principles and values as well as a formal policy platform, which the community will ratify with an up-or-down vote. Visit our Values & Policy webpage to see published articles, and our timeline for discussion. #MEActionVPI
Join our upcoming Community Call to discuss our values and tactics on Wednesday, October 30th at 10 am PT / 1 pm ET / 6 pm UK
For most of us myalgic encephalomyelitis (ME) is enduring, substantial and has a significant impact on our life. These are the very requirements of defining a disability.
Do you identify as Disabled, though? I find a surprising number of people with myalgic encephalomyelitis (pwME) don’t. I understand this, it took me 10 years to get to that place myself and for most of that time I was working with other disabled people. There are a number of reasons why:
It is emotional for everyone to come to terms with disability, and, with ME, other people don’t tend to label us as disabled; we hope to get better so don’t want to take on a marginalised self identity. We weren’t born with the disease (although, if we have a genetic predisposition does that change this thinking?). We initially got sick rather than injured so tend to think of ourselves as ill. Sometimes our symptoms are mild and not substantial; we are brought up to think of disabled as using a wheelchair and many of us don’t and, so on.
Does it matter? I think what conclusion you come to is your personal business and not for me to say. I shouldn’t define your identity for you. However, I think it is important enough an issue to warrant giving it serious thought. Benefits of identifying as Disabled include becoming part of a wider, more powerful community (1 in 5 adults of working age are disabled), taking advantage of disability rights against discrimination, claiming more benefits and disability discounts, contributing to wider debates about what it is to be disabled and making sure pwME are included.
Will you be Disabled when well? #MEAction’s co-founder, Jen Brea, made an interesting point on Twitter once that even when she’s well she’ll still identify as Disabled. I’d never thought about that before, but I think I’ll be the same.
It is important for me to hold onto internal narratives around, “When I am well, I will..,” which seems to somewhat contradict the concept of having a fixed, Disability identity. However, if identity is more of a way of seeing the world, then I won’t want to lose that when I recover. ME has changed me. I won’t be the person I would have been without it. Just as a queer person doesn’t lose the knowledge of a marginalised viewpoint or homophobia when they date someone of the opposite sex, I won’t lose my Disability identity if I became well.
Models of Illness and Disability
There are different theoretical models or perspectives used to understand illness and disability. These models are culturally constructed and people may not be conscious of using them. I think these models are worth discussing a bit more in this article in relation to ME and disability. In my opinion none of them are a good fit for us.
In brief, the Medical Model locates the problem in the body and locates the solution in the hospital or doctor. It can be seen as paternalistic and outdated, treatment is imposed on the patient. The Social Model locates the problem in society and locates the solution in changing attitudes or the physical environment. It tends to be the main view of disability charities, but is difficult to apply to impairment caused by illness.The Biopsychosocial Model potentially locates the problem in an interplay between the body, mind and society, but usually in practice locates the solution in individual thought and behaviour change. It can be misused as a cost saving exercise or as patient blaming, relocating responsibility from the State to the individual.
Medical Model
The attitude of the Medical Model is one that a lot of pwme would initially welcome. It situates the problem as within our bodies, so is conducive to biomedical research and being prescribed actual medicine. However, it is also the Model which locked up people who had learning difficulties for life in large hospitals. If you scratch the surface, I think the dynamic of doctor-patient relationship that springs from this way of thinking is unsatisfactory for pwME too. It fosters the kind of paternalism that is likely to dismiss patient experiences, especially if doctors haven’t done the right test to find where the problem is in the body.
Social Model of Disability
The Social Model is a grassroots, movement of the people as the theoretical backbone to the Disabled People’s Movement. This sounds more promising. However if you take a hardline stance on this model, the disabling problem can only be located at the society level, the problem to be fixed is never within the individual. This works if you have a specific, stable condition and are otherwise well (for example for amputees or people with a sensory impairment). Once society adapts to their needs then they no longer experience barriers to participation. Obviously full adaptation has yet to happen, but it is quite conceivable with the right commitment.
However, if there are no satisfactory adjustments to make society accessible for us it becomes a problem that tends to be avoided as an inconvenient truth. Post Exertional Malaise can’t fully be solved at the society level. There are things that could help: flexible hours, an accommodating benefit system, normalising working at home. When I was working on the Chronic Illness Inclusion Project I had all of these adjustments, and colleagues who understood my impairment, but nothing was sufficient to overcome severe energy restriction. People with ME actually do need to be fixed at the body level.
We need the Disabled People’s Movement to acknowledge the complexity of different types of impairment.*
Contributing to the Debate
I think this is a useful way to conceptualise how we fit in, as described by the Limited Capability blog.
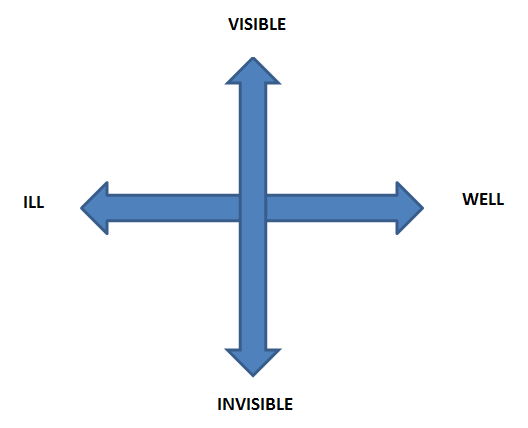
“The idea is this: all forms of disability/impairment* can be located along two axes: Well to Ill, and Visible to Invisible. Ultimately, the aim is to better distinguish what kind of adjustments people need in order to be included; and understand what kind of discrimination they may face.
The Disability Rights narrative has largely been mapped from the vantage point of the Well and Visible ends of the spectrum. The forms of prejudice and discrimination encountered from this position are relatively well documented. But social oppression and disablism is equally, though differently, experienced from the opposite vantage point: the Ill and Invisible ends of the spectrum.”
I think pwME have a role to contribute to the conceptualisation of disability in this way, and that will help those with rarer conditions who are disabled but not Well-Visible.
Moving forward: Advocating for “Energy Limiting Chronic Illness”
I have been involved in research** on the Chronic Illness Inclusion Project. The rationale for this project has been:
“Internet and social media have fostered a burgeoning community among people who identify as sick or ill (see also #spoonie), rather than, or as well as, “disabled”. People who, due to the severity of their symptoms, cannot access physical spaces of assembly or activism despite adjustments and adaptations, now have a medium for communication and participation.
As yet, this online community has no formally constituted, user-led organisation. It has no collective voice, broader than the individual diagnostic label, with which to resist and challenge the particular forms of restricted citizenship experienced by people with chronic illness. Their lived experience remains below the radar of policy makers and service providers.”
This lack of representation is a significant barrier to shaping the policies that affect their lives. It has been especially detrimental in the context of welfare “reform”. Under a flawed “biopsychosocial” model, people with long term physical and mental health conditions have been targeted by successive government projects to redefine disability and deservingness in order to reduce entitlements to social security. As a result, opportunities for independent living have reduced significantly for this group.
The need to gain visibility and legitimacy as a constituency of disabled people, and to have their voice heard by the broader disability rights movement and policy makers has never been more urgent.
This small project has combined qualitative and survey methods to explore issues around self identification and priorities for change. The results are yet to be fully analysed but will feed into a Manifesto style report.
From preliminary analysis it’s looking like energy impairment and energy-limiting chronic illness (ELCI, pronounced Elsie) are the preferred terms for self-identification among people with long-term health conditions similar to ME. This is a wider category of Sick disabled people who have the shared lived experience of needing to budget energy, or avoid change in routine, in order to manage symptoms. Essentially it is a policy maker, friendly translation of the term “spoonie,” which could form a meaningful grouping of conditions within the Disabled People’s Movement.
Conclusion
It is important to recognise that ‘difference’ can mean variation rather than tension and conflict (as Claudia Gillberg pointed out on Twitter). Most other disabled people do want to include us but they don’t have our lived experience. They need to hear our perspective on impairment, adjustments and priorities for change and we need to be represented when disability policy is discussed.
This is best achieved within a meaningful grouping of the various Energy Limiting Chronic Illness organisations and by us, as individuals, raising our voices inside the Disabled People’s Movement.
Visit our Values & Policy webpage to read published articles, see the timeline for discussion and join community calls. #MEActionVPI
About the Author: Jenny lives with fluctuating ME and other Energy Limiting Chronic Illness related impairment. During milder phases she has worked in the disability sector. Her most recent roles have been as a researcher for the Centre for Welfare Reform working on the Chronic Illness Inclusion Project and volunteering as a NICE (UK clinical guidelines) rep for #MEAction UK.
*A case in point: on my first day as a new employee at a Disabled People’s Organisation in 2011, there was a high profile disability activist speaker who claimed we should abandon low rate Disability Living Allowance (DLA) claimants to the benefit cuts as collateral in order to safeguard those with more severe disabilities. In the course of his speech he also talked about a case study of someone with severe fibromyalgia, and he was very sympathetic. I realised with frustration that as someone with a stable, physical disability he didn’t quite get that this could be the same person.
If you have fluctuating conditions like fibromyalgia and ME you can be one week at a Low Rate DLA level of functioning and the next in a relapse unable to get out of bed. I actually became a classic example of this: at the time of his speech on Low Rate Care, but within a few months qualifying for High Rate Mobility, Support Group ESA and bedridden. What really, really doesn’t help people like us is to be forced through financial necessity (benefit cuts) to work beyond our energy envelope, ending up in relapse.
**Research methods:
A combination of participatory action research methods and surveys will be used to develop the following research agenda in stages:
1.*Self-identification: What are the core features of the online community that unites under the banner of #spoonie #invisibleillness or “Sick”? How can this lived experience be made intelligible to those outside the community?*
2). Exploration of the social model of disability using Duffy’s “7 keys of citizenship” concept to prompt discussion about aspirations, autonomy, and dignity.
3) Identifying barriers: using the 12 pillars of independent living, prompt discussion of the attitudinal, organisational, environmental and political barriers to independent living.
4) The co-production of a manifesto for social change within the PAR forum.”



15 thoughts on “Are you Disabled? How does ME fit into the Disabled People’s Movement?”
Really excellent piece. Thank you.
I think this is really vital work.
What is the “PAR forum“ mentioned in the last line? I can’t find a reference for that in the article.
Thanks
Sorry, it shouldn’t have been abbreviated. It’s a type of research method- Participatory Action Research (PAR) – but not important for understanding this article
https://www.participatorymethods.org/glossary/participatory-action-research
I totally agree with defining an ‘elci group. With a clear identity comes clarity of purpose, and ultimately political clout.
ME/CFS sufferers need a strong identity.
Problem goes back to diagnosis, definition and reluctance of doctors to use all possible tests to find causes. Had my daughter been given a toxicity test for heavy metals by the GP at the first call she would never have had to spent 6 years in bed, nor to wrestle with severe mental health issues as she detoxed a high level of mercury. Warning to anyone with amalgam fillings – get them removed by an holistic dentist using all precautions.
Thank you so much, Jenny for your considered and erudite exploration of what it means to have myalgic encephalomyelitis. I particularly appreciate your comments about the tension between disability and sickness. I live in that space, forever hoping and, in every conceivable way, ‘working towards’ my recovery while, on a day to day basis, trying to cope with profound limitation and pain, both physical and emotional. I can’t bring myself to accept I’m permanently disabled yet, as the days turn to weeks, months, years and now a decade, I may somehow have to come to terms with my reality.
All the very best to you for the continuation of your wonderful work.
Jacqueline
Thanks. Accepting a disability identity doesn’t necessarily also mean giving up on a future that no longer contains ME. It doesn’t have to mean accepting a permanent, fixed level of impairment. In that way the uncertainty of ME can be seen as a weird advantage compared to many other conditions. Most of us have no idea what the future will hold will hold with ME, it’s unusually fluctuating, and there could also be research breakthroughs. But I think it is accurate to say we have a condition which is substantial and enduring (a disability). Impairment doesn’t have to be at a fixed level of severity to think of yourself as disabled.
It is also ok to not think of yourself as disabled.
Calling oneself disabled are you’ve recovered from an illness and are able-bodied and able to function at a job and in daily life independently (in the quote from Jen the author agreed with) is appropriation, it’s pretending that being disabled is an identity politic, and it’s offensive, just as it’s offensive for mild or moderate ME patients to call themselves “severe” ME patients versus severely disabled. As Susan Sontag aptly stated, “illness is not a metaphor,” and treating it a metaphor, ideology, or simply an idea versus a gritty lived reality one can “put on” is what leads and re-leads us to ableist oppression. The same grounds for offensiveness also apply in parallel forms to Rachel Dolezal calling herself black because she feels she has a black identity when she’s white (instead of owning her white privilege), a tourist to a refugee encampment calling oneself a refugee (instead of owning the privilege of being born into fortunate citizenship), Elizabeth Warren misinterpreting genetics for tribal membership, or even me saying that since I went to Newtown once, I totally get what it is to be Newtown Strong (when I never lived through that horror). None of these are the same as, say, calling oneself queer if one isn’t currently in an obviously queer relationship. With the queer community, the need to claim this (“we’re here, we’re queer, we’re fabulous, get used to it!”) was and is a response to a completely different set of politics.
It isn’t okay for someone in a leadership position in ME who *is* recovered to identify as “disabled” still: Jen is “temporarily abled,” and could call herself that or an “ally” or both, but she’s not disabled. There are a lot of places to be a model ally, or a person recognizing the privilege of recovery or being temporarily abled, but turning that into the Oppression Olympics (“I’m disabled too!” or even “I’m disabled still when I’m not, for solidarity!”) will never serve the sickest, most disabled patients.
I agree that mapping out invisibility versus non-invisibility, and well/sick poles is a good way to define the subset you’re talking about — and I love the idea of “Elsie” to unify conditions that impair energy. But it also isn’t true that this hasn’t been regularly addressed in the ME community and even the disability community — I was invited to speak on this topic (invisible disability versus visible disability) at a disability conference by video around 2000 (as an ME patient), and a lot of others have carried this same torch. The disability community has and will happily embrace us, it’s just that it’s also true policy on invisible or non-apparent disabilities (especially around services) lags far far behind, and the medical versus social model creates a rock and hard place for many of us still hoping for recovery.
Disability is an important medical designation for life-saving services like caregivers that many of us rely on for life and death, and though the definitions desperately need to be expanded to better serve the needs of waxing-and-waning disabilities, invisible disabilities, and others that don’t fit as easily into fixed equations, this still doesn’t mean allies should call themselves disabled and further the abstraction of what disability actually is.
Peggy
Thank you for engaging with these ideas and discussing them. I think provoking discussion, and from that writing policy, is the aim of this collection of articles.
Something that is probably worth mentioning is I wrote most of this article 3 years ago before Jen Brea’s recent medical breakthroughs (it was a post on my blog I was asked to edit for the value and policy articles at the end of 2018, IIRC before I knew that Jen was in remission from ME and POTS). It was 2015 or 2016 when Jen made that comment. I don’t know what her opinion is now she has lived experience of this dilemma, that would be interesting to know.
My perspective is I’d like to challenge how we define disability, so that it does fit the experiences of people with fluctuating chronic illness (which can go into remission) and whose impairments aren’t entirely overcome by society level adjustments. I don’t want to accept the grammar of disability politics if it doesn’t fit the experiences of a large section of the disability community. As someone who is queer and disabled I see them as pretty similar types of identity experience. It is identity politics.
I don’t think anyone can randomly (legitimately) claim to be disabled though, they need to have had experience of “substantial, adverse, and long-term effect on ability to carry out normal day-to-day activities” (UK Equality Act 2010 definition). I’m talking in the context of people who are for long stretches of time clearly meeting impairment criteria for disability, but who might not experience that for the rest of their lives, either going in and of remission or at some point receiving effective treatment. I feel it is inappropriate to call this appropriation.
Interestingly, people with mental health issues are covered under UK Equality law even when well (as long as they previously met the disability definition threshold). This is something I think should be extended to ELCI conditions. It also shows this way of seeing disability has been accepted in other contexts. In remission you don’t lose all the obstacles you experienced when seriously ill. Your career has still been disrupted, for example, and potential employers are likely to reluctant to hire someone who’s been on disability benefits for years. If we still experience oppression related to health and disability we are to some extent still disabled, even if there is no current impairment. This isn’t a metaphor, but it is more about social oppression than medical status. Again the different models of disability competing!
I agree that the disability community feels happy to want to embrace us, but in my experience from working in UK disability charities, our experience of impairment is very challenging to how other disabled people want to talk about disability. For example, a recent discussion in the Chronic Illness Inclusion Project is around the terms housebound and bedbound. We tend to use these as descriptions of severity, but people who adhere strongly to the Social Model are upset by that and want someone being housebound to be a starting point for campaigning to get the adjustments and support so that people can leave the house. Independent living is a big emphasis. In contrast, we would probably want it to be a campaigning point for medical research and treatment, and in the meantime accessing social care to stay at home (because in our case there aren’t adjustments which overcome the impairment).
Also, I don’t know if this will be covered in a different article, but it would be good for this V&P process to include discussion of how we respond as a community to people going into remission through effective treatment (or natural fluctuations ). My personal response would be to still consider them a pwme who is currently in remission, rather than having people feel they have to re identify as an ally of pwme.
I’m really hoping that this will become a big issue to deal with in the sense that more and more of us will discover the underlying cause of our ME and receive effective treatment. There’s a likelihood that this will be in a series of subgroups rather than everyone getting well at once. How would we want people to respond if we happen to be the first, or the last subgroup?
I do not feel comfortable debating in a forum anywhere, but especially here (an organizational space Jen founded!), the self-stated identity as disabled of Jen Brea. Nobody gets to debate or define Jen’s identity except Jen. It’s dehumanizing to do so.
This discussion does raise larger questions about disability as a political identity. For people with ME, disability as identity is borne from our experiences in a society that disables our bodies (the social model) by way of institutions, policies, practices, prejudices (etc.) that shape the daily lives of the sick and chronically ill. I think this understanding goes beyond the idea that queer is queer no matter who you’re sleeping with (note to author: queers don’t traffic in binaries, so “opposite sex” is not the right metric to use). Disability as identity means once you have experienced the heavy weight of disability, it never leaves a body. If I had a “cure” tomorrow, as someone who has lived with this condition for 35 years, i would always and ever identify as politically disabled. As a trans person who has medically transitioned, I am not no longer a trans person; I am still trans. Trans is the better analogy than queer, as it is used in this article, to demonstrate why identities persist despite a (possible) change in physical status.
Perhaps it’s also helpful to think about disability and identity the way disability activist Mia Mingus talks about it. Mingus describes “descriptively disabled” but not “politically disabled” as someone who has experienced ableism but does not necessarily have an “analysis about ableism, power, privilege” or feel “connected to and…in solidarity with other disabled people.” Not everyone who is descriptively disabled is politically disabled; however, once one identifies as politically disabled nobody has the right to take that away.
Thanks for engaging this important conversation about labels and privilege, I agree it’s an important one. My general feeling is that calling oneself disabled, even “politically disabled” is a far cry from calling oneself a PWME in remission or recovered or an ally. I would in fact argue the opposite point to Ben’s point here: I would argue it’s completely dehumanizing to people who are still living the physical reality of disability (versus the ensuing grief and trauma of having lived through it) to call oneself “politically disabled” and appropriate the language of disability. It feels dehumanizing to ME, personally, to hear that people would do this — but also, censoring dissent around it or calling dissent or critique itself dehumanizing would be a mistake in terms of what this values and policy initiative stands for.
Certainly, a third category could exist, one between disabled and temporarily abled or ally (and we could invent a new language for it), but I have to strongly disagree that Jen or another recovered person has the right to take the language of “disabled” and use it (and, notably, in 27 years of being sick, I don’t think any very-sick ME patient I know of who has recovered would ever do this): it dehumanizes those of us fighting tooth and nail to get social services to recognize the level of that word we are living with, and how many home health aide/PCA hours we need to keep breathing, and it’s just politically dangerous for the still-very-sick given the long history of misleading language, metaphor, and ensuing violence against this illness. I think another analogy would be a long-time prisoner released on new DNA evidence after serving time for a crime he didn’t commit. He will see himself as a released prisoner (with the experience inevitably having changed him), not a prisoner living the life of those who may never get out. He is no longer the same as his friends still in prison, and that distinction absolutely matters, and he would offend them by calling himself then a “political prisoner,” which we all know already has a different meaning entirely. It’s just not solidarity to appropriate someone else’s currently-lived experience: it’s appropriation. That person has every right to call himself a “politicized ex-prisoner” working in prison rights, and he may have significant trauma or organic brain changes induced by prolonged imprisonment, but he’s not a prisoner any more.. But the language and — more importantly — the political implication of that language matters.
I know Mia Mingus’ work and very much respect it, but would be very surprised if that was the point she was making (that a non-disabled person can be “descriptively disabled” and/or “politically disabled” versus a still-disabled person using those terms — I’d love a link to what you’re referring to). I thought of another analogy: people who call themselves “trans-abled,” that is, people with a paraphilia who induce disability or pretend to be disabled and use wheelchairs because they FEEL an identification with disability and fetishize disability. I’d strongly argue it’s not their “right” to self-label as such, and the disability community has generally fought against their “right” to do that, and I’m guessing the trans community has too. “Trans-disabled” is a paraphilia based on power, control, and appropriation.
As someone living within ME and disability for 27 years, well over half my life now, it’s hard to imagine what an emergence from this illness would feel like now, and in asking recovered people who it has felt like for them, I have been surprised mostly that they’re not riddled with fear of a relapse. But none of them still call themselves disabled, and as activists and intellectuals and people with an astute analysis on this, I don’t think any of them actually would.
It IS good to know that Jen made that comment about still calling herself disabled if recovered before her recovery, as maybe her viewpoint is different now: but I think as a figurehead in the community, she should be backpedaling on that (offensive) remark now and making a clear statement on how she stands at the point of having had the luck/fortune/ability to recover if we’re talking about privilege and owning privilege, because this *is* an acquired privilege (recovery) and she should just own it as such. Owning it doesn’t state that she never lived through the hell of ME for years; it’s simply stating that she’s not in the same place as her friends still in prison, she’s not “a prisoner” now, she’s an ally or something else if she wants to be. In my opinion, owning luck or good fortune is about owning privilege, and she (or anyone recovered) should not continue to call herself politically disabled as if disability is more a politic than a gritty lived reality of fighting for survival for many people — a “politicized disability ally,” sure, but that’s not the same thing. I do think the words matter. And I think “politically disabled” is not just a misuse of the language of disability, but that it has potential to cause enormous harm to disabled folks who are already fighting inspiration porn in the media and a lot of people malevolently using psychogenic theories and bogus language-based projections to contain and control us.
I completely agree a transperson has every right to call him/her/themselves trans whether they have surgery or take T or use a binder or not (and I’ve had occasion to fight for friends living those realities), but these are just not the same things. I’ve been writing and publishing in the queer community and the ME community for over 20 years, the conference I mentioned where I spoke via video on invisible (non-apparent) versus visible (more apparent) disabilities was a queer disability conference, I was censored as a Lambda Literary finalist because my work was considered so queer it seemed almost straight due to a use of male pronouns that freaked out a transphobic Lambda official (an incident that also had a lot to do with disability invisibility). But, given this personal history, I’d argue that it’s a privilege to be in a physical state where one *can* challenge or question designations many of us cling to for dear life (like “disabled”) because if we didn’t, we wouldn’t have any money for food or rent, or we would in no way qualify for the caregiving services that allow us to keep breathing. It’s a vastly different thing to say, instead,”I got really really lucky, I’m temporarily abled, I’m in remission, I’m not disabled right now” or even “I’m in full remission, but statistically I could always relapse” versus taking from those of us who are this far down the label that actually keeps us alive. And to me, that’s the privilege a recovered person should own. In ME, we do actually know from long-time doctors/observers like Dr. Cheney that — like MS — we may have three distinct groups, groups that go along three trajectories that he once described in a lecture: those who recover are slowly going up all along, those who stay the same are slowly on a flat line all along, those who get worse are slowly (or rapidly) getting worse all along. It’s just three lines on a graph, like an airline map, and isn’t about identity, grit, will, or intention. I would argue that more often than not, people know from early on which line they’re on, they feel it in their bodies, and it’s usually those in the more-fortunate group of thirds who think they did something to make it so. If one thinks he did something extremely special to get onto that recovering group and then fortunately ease out of it into a recovery or remission, that’s privilege. That’s the legacy student at Harvard thinking his enormous parental contribution and fake water polo pictures make him the same as the person who was shut out, or the person who really earned it. So we can’t minimize the danger of that, politically. If this overriding discussion is actually about dissecting privilege, we have to dissect what taking on this word (“disabled”) then means for those who have the privilege to experience temporary-abled living again. It’s not that they won’t live through the trauma of this experience forever, I have no doubt, it’s just that the minute they are well and the rest of us aren’t, they are *immediately granted* a lot of privileges that able-bodied people get, often by virtue of their bodies having a certain amount of ability to navigate their world at will.
So I’d strongly challenge people in this community to really question the logic of continuing to use the term “disabled” and be okay with that, post-recovery. I don’t agree it’s everyone’s right to “self-identify” that way, not in places or countries where social services or medical care are often parceled out at a non-life-sustaining level (or not at all) to people who “qualify” as disabled per the fairly rigid standards that simply exist, I think it’s then taking on the identity of a marginalized group to skew the distribution of goods and services and accommodations people need to function and survive. It also, as one ally pointed out to me, indicates that there is something wrong or inferior about moving into becoming an “ally,” or “temporarily abled,” or some other third label designation we haven’t come up with (or allies or recovered folks haven’t come up with) yet. This ally noted to me that allies need to see models of real ableism-fighting allies too (whether recovered or just “temporarily abled”), they need to see allies to the community who are *using their able-bodied or temporary-able-bodied privilege* to do good, by first owning what that is (able-bodied privilege), and then being proud to call themselves allies and fight their own internalized ableism (which we all have to do). So why not elevate the idea that able-bodied people (even if temporarily abled) can have deep empathy, care for the sick, be disability activists (versus “politically disabled”) and identify from the vantage point of allies? In my opinion, this would have to start with more honestly owning the privilege of recovery too.
thank you so much for your words and your work, jenny. i identify as a person with ME (pwME), a person with energy limiting chronic illness (elci), a person with fluncutuating ME, a person who is sick and disabled. i think the more ways we can identify as individuals, the more intersections and connections can be made with each other and the wider world. there is more that unites us than divides us.
I thought this piece of writing was very thoughtful and addresses an important aspect of how people with ME/CFS can “thrive rather than just survive” by defining and having society/community understand and accept our legitimate needs. I personally have been able to tell people exactly what I need “I can do this , this and this, but could use help with this”. I find however that very few people take this seriously , especially when my needs (even when small) are multiple and vary. Are you weak, or do you have a hearing sensitivity, or do you have food allergies, or catch colds/flu easily ? It seems any 1-2 of these would be considered legitimate & understandable, but when so many are factors AND some of them wax/wane ……..the majority of people conclude that I am a hypochondriac , attention seeking , “nuts” or even if real ……it’s too strange for them to want to know about. I have one neighbor that opens bottles for me that I can’t do. That’s one thing and she can handle that.
Soo there is much to do to enlighten society/communties/resouces how they can help. It is very frustrating to know what you need to greatly improve your quality of life, sometimes with very little help but be unable to get anyone to understand.
This is a follow up reply to one I did earlier. It is about the financial challenges that ME/CFS pose in addition to the rest. Many contract this condition in their 40s (or even younger)…..I was 43 yrs old and had to stop working and was lucky to receive SSDI . SSDI is barely enough for most to live on even if they had no out of pocket medical —-but people w/ME/CFS , often with food allergies , often with chemical sensititives, and often having to seek health providers that do not take insurance ……. typically have VERY HIGH OUT OF POCKET MEDICAL/HEALTH EXPENSES. Often they start by using up what nest egg they have at this young age ………hoping to fully recover and return to work. I have in the 25 yrs I have had ME/CFS been unable to SAVE a penny, and by cutting corners just manage to make ends meet …..each year finding less corners to cut.
Now……..there are various tasks that if financially better off I could hire help . And when I look to traditional support services available for typical disabilities or Seniors or low income …….I some how don’t quite meet these categories. Some for the simple reason that you need to STAND IN LINE, some because my income is just ABOVE poverty level …..(if factoring in out of pocket medical costs it would be quite BELOW poverty level but things like vitamins, supplements, gluten free foods , homeopathics instead of flu shots, and the list goes on………… are often not taken seriously as legitimate “out of pocket medical
expenses”.
My point is that our population not only need support services, but need financial assistance, if only to help with out of pocket medical expenses and mainstream organizations need to be made aware and seriously consider this.
I am reminded of the stereotypical illustrations of Blind and other Disabled people selling things and people happily buying “for such worthy cause”. I have tried to sell some things I own , hoping to get a fair price or even a bit more (as I am a “good cause”)….but people assume I must be well off if I haven’t worked in some years …..and want me to sell such items at “fire sale prices”….after all “I look fine”.
(My career background is in helping profession, not business ,so my personality is better at “giving then selling” and that doesn’t help either !)
There are just so many factors that challenge a person with ME/CFS from living their best life – even with their medical condition . I’ve heard thru the years several labels instead of “Disabled” that would be more comfortable a fit for ME/CFS…… “differently abled”, “marginally abled”, and a few others I can’t think of at the moment that are even better.
Financial hardship is common for most disabled people. It is a shared experience. However, there can be different perspectives on the correct response, depending on your wider political beliefs and concept of disability.
If you’re feeling well enough to read it, this paper is interesting re linking agendas to cut welfare money and how UK ME research ended up in the mess it’s in https://www.centreforwelfarereform.org/library/in-the-expectation-of-recovery.html
Comments are closed.